WORKING GROUP DRAFT – IN CONFIDENCEReport on Government Services 2026
PART E, SECTION 10: RELEASED ON 5 FEBRUARY 2026
10 Primary and community health
This section reports on the performance of primary and community health services which include general practice, pharmaceutical services, dentistry, allied health services, community health services, maternal and child health and alcohol and other drug treatment. This section does not include:
- public hospital emergency departments and outpatient services (reported in section 12, ‘Public hospitals’)
- community mental health services (reported in section 13, ‘Services for mental health’)
- home and community care services (reported in section 14, ‘Aged care’ and section 15, ‘Services for people with disability’).
The Indicator results tab uses data from the data tables to provide information on the performance for each indicator in the Indicator framework. The same data is also available in CSV format.
Data downloads
![]() 10 Primary and community health data tables (XLSX 905.6 KB)
10 Primary and community health data tables (XLSX 905.6 KB)
![]() 10 Primary and community health dataset (CSV 2.7 MB)
10 Primary and community health dataset (CSV 2.7 MB)
Refer to the corresponding table number in the data tables for detailed definitions, caveats, footnotes and data source(s).
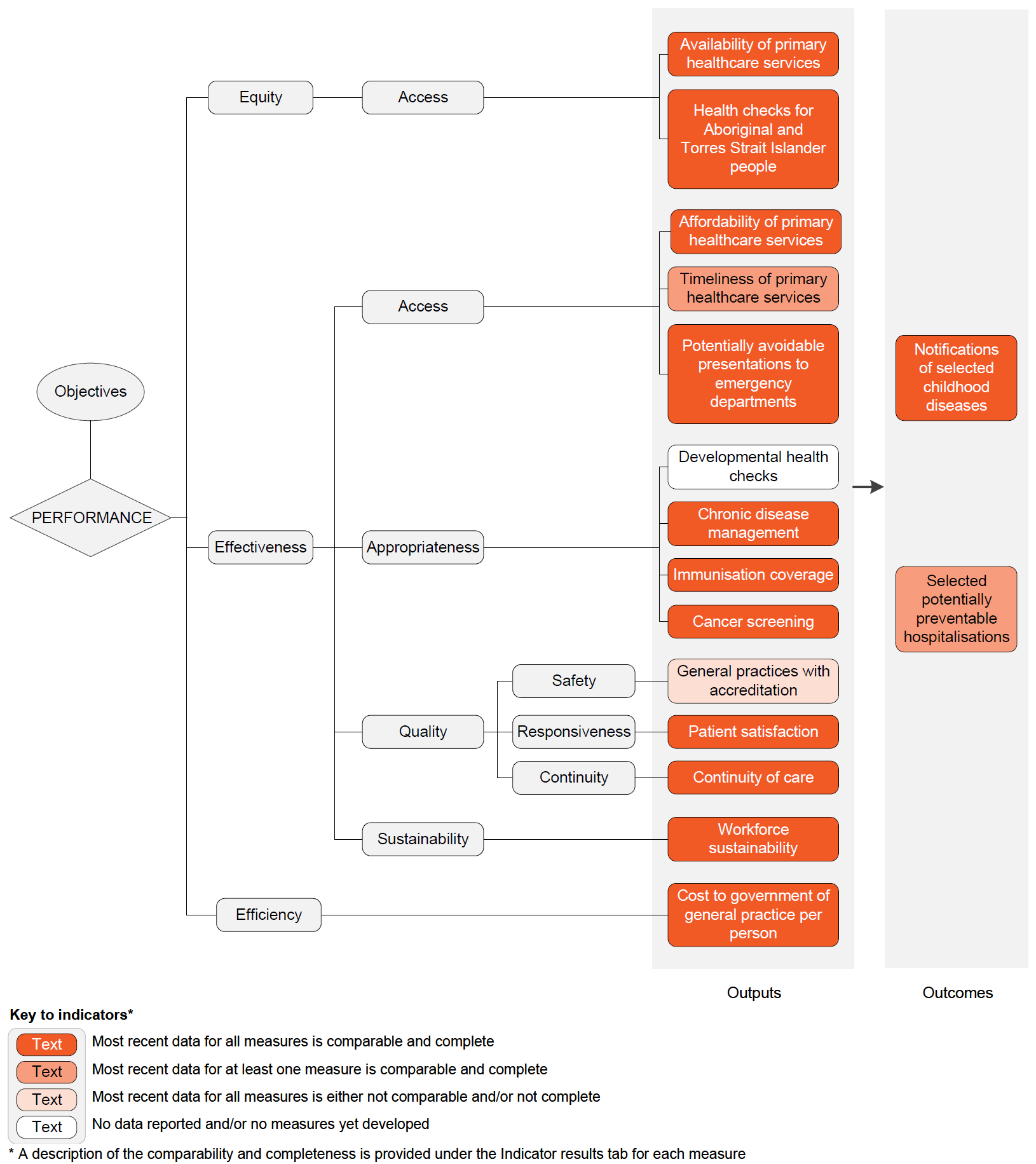
Objectives for primary and community health
Primary and community health services aim to promote health, prevent illness and support people to manage their health issues in the community, by providing services that are:
- timely, affordable and accessible to all
- appropriate and responsive to meet the needs of individuals throughout their lifespan and communities
- well coordinated to ensure continuity of care where more than one service type, and/or ongoing service provision is required
- sustainable.
Governments aim for primary and community health services to meet these objectives in an equitable and efficient manner.
Primary and community health services are delivered by a range of health and allied health professionals in various private, not‑for‑profit and government service settings. Definitions for common health terms are provided in the 'Explanatory material' tab.
General practice
General practice is a major provider of primary healthcare in Australia. General practice services include preventative care and the diagnosis and treatment of illness and injury, through direct service provision and/or referral to acute (hospital) or other healthcare services, as appropriate.
The Australian Government provides the majority of general practice income, through Services Australia – mainly as fee-for-service payments via the Medicare Benefits Schedule (Medicare) – and the Department of Veterans’ Affairs (DVA). Additional funding is provided to influence the supply, regional distribution and quality of general practice services, and support engagement of the health workforce in primary health care settings, through initiatives such as the Practice Incentives Program (PIP), the Workforce Incentive Program (WIP), and Primary Health Networks (PHNs) (Services Australia 2021). State and territory governments also provide some funding for such programs, mainly to influence the availability of General Practitioners (GPs) in rural and remote areas. The remainder comes primarily from insurance schemes (for example, workers compensation schemes and traffic accident schemes that cover medical expenses in certain circumstances) and patient contributions.
Pharmaceutical services
The Commonwealth funds the Pharmaceutical Benefits Scheme (PBS), which subsidises the cost of many medicines in Australia. The PBS schedule sets a price for listed medicines and a maximum co-payment amount that people contribute towards the cost of these medicines. The Commonwealth incurs the expense of any difference where the listed price exceeds the patient co-contribution (whether for general or concessional patients).
Around 69% of PBS prescriptions dispensed in 2022-23 were above the co-payment threshold, meaning patients paid the relevant co-payment and the remaining cost was subsidised by the Australian Government. Around 31% of PBS prescriptions dispensed in 2022-23 were under the co-payment threshold, meaning the patient paid the full cost with no government subsidy (AIHW unpublished). Co-payments contribute to a patient’s safety net threshold that, once reached, provides eligibility to receive PBS medicines at a lower cost or free of charge (Department of Health and Aged Care 2021).
The Repatriation Pharmaceutical Benefits Scheme (RPBS) provides subsidised pharmaceutical medicines, dressings and other items to war veterans and war widows. The RPBS is administered by the DVA.
Dental services
Australia has a mixed system of public and private dental services. State and territory governments deliver public dental services, which are primarily available to children and disadvantaged adults. The Australian Government works with state and territory governments to fund dental services. Since 2013, the Australian Government has increased funding for public dental services via National Partnership Agreements and Federal Funding Agreements with states and territories and the Child Dental Benefits Schedule. The private sector receives funding to provide some public dental services from the Australian Government through the DVA and the Child Dental Benefits Schedule, and from state and territory governments through dental voucher systems. Under the COAG Health Council, Australian governments developed the National Oral Health Plan 2015 to 2024 that sets out priorities to improve dental health across Australia (COAG 2015). Data on dental service expenditure in 2023-24 is presented in table 10A.6.
Allied health services
Allied health services include, but are not limited to, physiotherapy, psychology, occupational therapy, podiatry and osteopathy. They are delivered mainly in the private sector. Some government funding of private allied health services is provided through insurance schemes and the private health insurance rebate. The Australian Government makes some allied health services available under Medicare to patients with particular needs – for example, people with chronic conditions and complex care needs. The Australian Government also funds the Workforce Incentive Program (WIP) – Practice Steam, which supports general practices, Aboriginal Medical Services and Aboriginal Community Controlled Health Services with the cost of engaging eligible allied health professionals. Data on the number of Medicare rebated allied health services used per person and the availability of public allied health professionals by region is presented in tables 10A.10 and 10A.22, respectively.
Community health services
Community health services generally comprise multidisciplinary teams of health and allied health professionals who provide targeted health promotion, prevention and management services. Their aim is to protect the health and wellbeing of local populations, particularly people who have or are at risk of the poorest health and/or have the greatest economic and social needs, while taking pressure off the acute care health system. Governments (including local governments) provide community health services directly or indirectly by funding local health services and community organisations. There is no national strategy for community health services and there is considerable variation in the services provided across jurisdictions.
State and territory governments are responsible for most community health services. The Australian Government is primarily responsible for serving Aboriginal and Torres Strait Islander communities, with state and territory governments also providing some funding.
Maternal and child health services
Maternal and child health services are funded by state and territory governments. They provide services including: parenting support (including antenatal and postnatal programs); early childhood nursing programs; disease prevention programs (including childhood immunisations); and early intervention and treatment programs related to child health and development. Some jurisdictions also provide specialist programs through child health services, including hearing screening programs, and mothers and babies residential programs.
Alcohol and other drug treatment
Alcohol and other drug treatment activities range from a brief intervention to long-term residential treatment. Types of treatment include withdrawal management, pharmacological treatment, counselling and rehabilitation. Selected data on these services is available in table 10A.13.
In 2022-23, of the $50.3 billion government recurrent expenditure on primary and community health services, almost three-quarters was funded by the Australian Government and one-quarter by state, territory and local governments (table 10A.1). This included:
- $11.8 billion for community health services (18.3% by the Australian Government and 81.7% by state, territory and local governments)
- $2.4 billion for dental services (57.7% by the Australian Government and 42.3% by state, territory and local governments) (table 10A.6).
Where more recent data is available, for 2023-24, Australian Government expenditure was:
- $12.2 billion on general practice (table 10A.2)
- $18.1 billion through the PBS and RPBS on Section 85 prescription medicines filled at pharmacies (table 10A.3)
- $55.8 million on funding of PBS medicines to Aboriginal and Torres Strait Islander primary health services in remote and very remote areas (table 10A.5)
- $909.0 million on Aboriginal and Torres Strait Islander primary health services (table 10A.7).
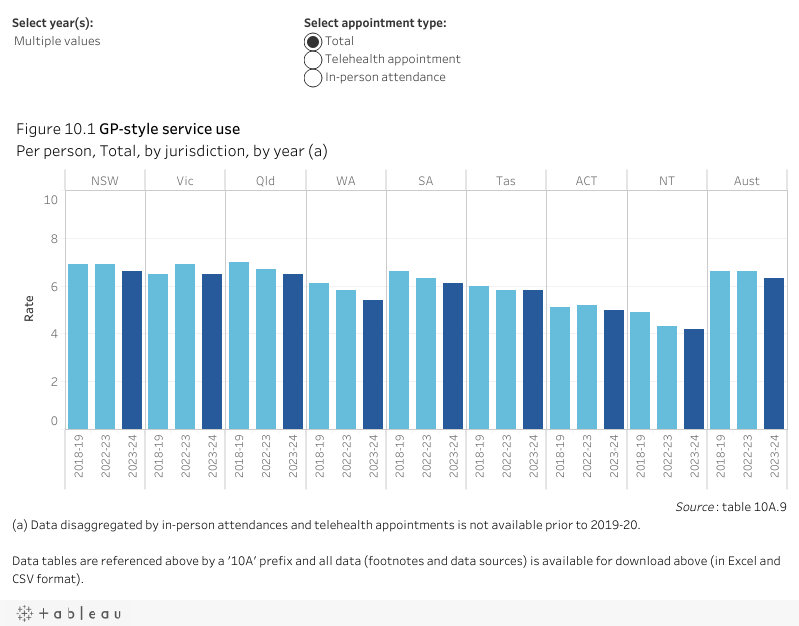
Nationally in 2023, there were 39,449 GPs – 29,215 on a full-time equivalent (FTE) basis, equating to 109.7 GPs per 100,000 people (table 10A.8), a decrease from 115.2 in 2022 (table 10A.8).
Nationally, rates of GP-type services used per person decreased between 2022-23 (6.6 services per person) and 2023-24 (6.3 services per person) (table 10A.9). GP-type services disaggregated by in-person attendances and telehealth appointments are reported in table 10A.9. Nationally in 2023-24, 1.0 telehealth GP-type service was used per person (figure 10.1).
Around 226 million services (8.4 per person) were subsidised under Section 85 of the PBS in 2023-24 – with 87.8% concessional. A further 7 million services were subsidised under the RPBS (tables 10A.11–12).
Nationally in 2022-23 there were:
- 213 Aboriginal and Torres Strait Islander primary health services which provided 3.7 million episodes of healthcare (table 10A.14). Data by remoteness is presented in table 10A.15 and health service staffing numbers are provided in table 10A.16.
- 1,280 alcohol and other drug treatment agencies (31.0% identified as government providers) with a reported 235,461 closed treatment episodes (26.8% identified as government provided) (table 10A.13).
The most recent available data on public dental service usage is for 2013 and showed that nationally, around 97.8 per 1,000 people accessed public dental services that year (AIHW unpublished).